Productivity in UK healthcare during and after the COVID-19 pandemic
Apr 22nd, 2021
Productivity in UK healthcare during and after the COVID-19 pandemic
As UK healthcare starts to recover from the pandemic, a new working paper from The Productivity Institute – Productivity in UK healthcare during and after the COVID-19 pandemic by Professor Diane Coyle, Kaya Dreesbeimdieck and Annabel Manley, of the University of Cambridge, explores the developments in NHS hospitals since March 2020, and looks at the impact of COVID-19 treatment pressures along with substantial falls in non-COVID-19 health care activities on measured productivity.
Based on a series of interviews (conducted in November and December 2020) in two English hospital trusts, as well as official health output figures, the paper highlights the impact of limited capacity in the NHS, including from the perspective of healthcare employees who worked during the peak of the pandemic.
It also asks how to think about and measure productivity in healthcare going forward, taking into account both the use of new technology in the past year, and the impact of the pandemic on health care activities. The authors argue that the NHS should be considered as a part of the nation’s infrastructure, with implications for additional capacity to insure against future health crises.
How should we measure productivity in healthcare?
As the numbers of treated and recovered COVID-19 patients increased and new treatment recommendations were made during 2020, the NHS required all hospitals to return to between 80 and 100% of baseline surgical activity by the end of the year. However, the interviewees raised concerns about the feasibility of meeting those targets:
“To me, this just seems completely out of kilter with what we should be doing. So, should we be only delivering the surgery on patients with the highest clinical priority, or should we be doing high volume numbers? And I think that’s very difficult for this organisation to make that decision.”
The interviews revealed that the rapid organisational change hospitals underwent in the early stages of the pandemic were successfully enabled by:
Major buy-in by the internal and external NHS workforce
The provision of significant extra funding
The relaxation of governance processes
The creation of surge capacity
Setting up enhanced communication and technology infrastructure
Yet there was still a decrease in measured productivity. Some of this reflects the decrease in non-COVID-19 treatments, and uncertainty about what weight to put on different treatments in the statistical totals. However, there are also downward pressures on productivity due to lasting changes in the use of physical space in hospitals including for the “donning and doffing” of PPE and reconfiguration of wards to embed infectious disease control requirements.
The changes will reduce their effective capacity (in-patient and out-patient) in current facilities making requirements like a return to between 80 and 100% of baseline surgical activity very difficult.
The paper argues that UK healthcare productivity should not be measured by just by the conventional statistics but should also take into account broader economic welfare, including, “the insurance value of better infectious-disease control in a world at risk of experiencing repeated pandemics; the option value of a capacity margin in the event of other types of unexpected peak load demand; and the demand-reduction effects of better preventive care.”
Measurement of output vs measurement economic welfare
The UK’s health output performance was worse in terms of the published statistics than in some other countries, partly because of differences in the methods used, but also partly because limited capacity reduced non COVID-19 health activities so considerably. Nevertheless, the NHS response to the pandemic was essential for economic welfare.
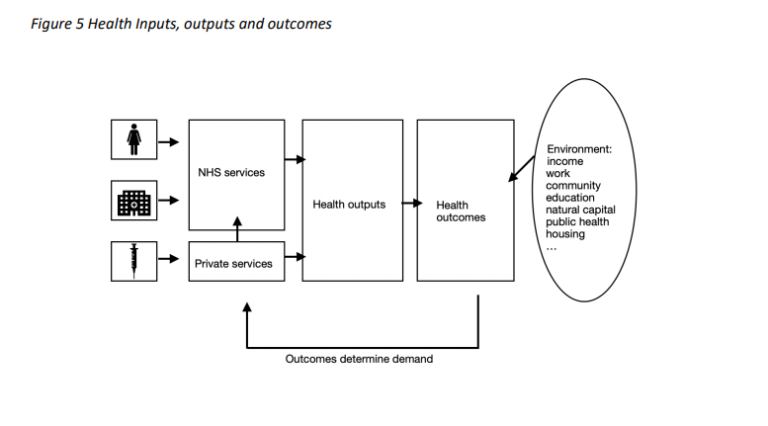
Future productivity improvements will require both adequate resources and use of new technologies such as video consultations or remote monitoring – but introduced with care, both to evaluate patient outcomes and to avoid a digital divide. Other factors including public health and the environment in which people live will also affect the productivity of the health service.
Authors Diane Coyle, Kaya Dreesbeimdieck, Annabel Manley (The University of Cambridge)
D. Coyle , K. Dreesbeimdieck , A. Manley (2021) Productivity in UK healthcare during and after the COVID-19 pandemic. The Productivity Institute working paper No.002
This website uses cookies so that we can provide you with the best user experience possible. Cookie information is stored in your browser and performs functions such as recognising you when you return to our website and helping our team to understand which sections of the website you find most interesting and useful.
Strictly Necessary Cookie should be enabled at all times so that we can save your preferences for cookie settings.
If you disable this cookie, we will not be able to save your preferences. This means that every time you visit this website you will need to enable or disable cookies again.
Analytics Cookies
This website uses Google Analytics to collect anonymous information such as the number of visitors to the site, and the most popular pages.
Keeping this cookie enabled helps us to improve our website.
Please enable Strictly Necessary Cookies first so that we can save your preferences!